
News & Events
Wave 2: Module 3: Aortic Week 5 – Case 1
16 year old male, presented to A&E following a road traffic accident.
HR 135, SBP 70mmHg, placed in a cervical collar and pelvic binder and no visible open fractures in upper or lower limbs
CT traumogram shows the following:
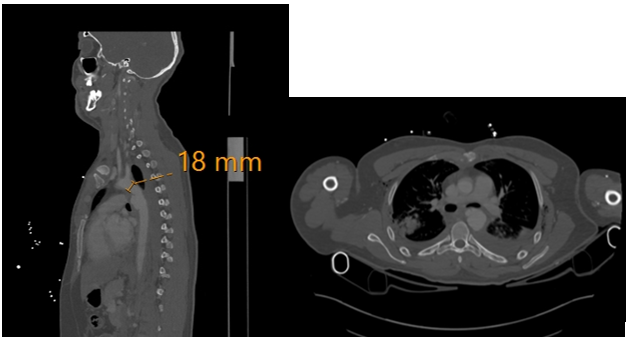
Q1: What is the most likely diagnosis?
Q2: What are the treatment options?
Q3: What are the technical considerations in planning this case?
8 Comments
Leave a Reply
You must be logged in to post a comment.
Q1 Traumatic type B aortic dissection
Q2 either conserve if only intimal tear is present, if the patient is unstable then surgical repair if the endovascular device is not available or unsuitable or TEVAR
Q3 the zone, the access vessels, the proximal landing zone, the aortic diameter
A1. Traumatic aortic dissection
..
A2 resuscitation and permissive hypotension
And TEVAR or open surgical
According to case
…
A3
In TEVAR
Check
Access vessel if small use iliac conduit
Landing zone 2cm from Lt subclavian and intmal flab should be covered to avoid leak
Q1:
Traumatic aortic injury is usually more of a transection rather than a typical dissection. Most of the time, it happens around the isthmus, just after the left subclavian artery. On imaging, it might look like a dissection, but it’s not the same thing — different mechanism and different approach.
⸻
Q2:
We usually start with permissive hypotension to control the bleeding, especially if the patient has other injuries. After stabilization, the definitive treatment would be either TEVAR or open surgical repair, depending on the case. We follow EVES guidelines for the decision-making.
⸻
Q3:
Before doing TEVAR, we need to check a few things. First, the access vessels — if they’re small, we might go for an iliac conduit. Then we need good landing zones, especially proximally, like at least 2 cm from the left subclavian. Also, the intimal flap should be completely covered to avoid leaks or any future problems.
A1: Traumatic Aortic dissection
A2: Immediate resuscitation with permissive hypotension and pain management.
TEVAR according to EVES guidelines
A3: Access vessels with possibility of iliac conduit having to be used due to smaller caliber vessel size
Proximal landing zone 2 cms away from LSA
Coverage of intimal flap
Q1:
traumatic aortic injury mostly type aortic dissection
Q2:
permissive hypotension then
open surgical repair of the aorta or TEVAR according to EVES guidlines
Q3:
access vessel of appropriate size and as the patient may has small vessel size an iliac conduit may be used
landing zones proximal and distal wit proximal landing zone 2 cm from left subclavian artery
full coverage of the intimal flap
Q1: What is the most likely diagnosis?
the most likely diagnosis is traumatic aortic injury (TAI), specifically a traumatic aortic dissection.
Q2: What are the treatment options?
* Thoracic Endovascular Aortic Repair (TEVAR)
* Open Surgical Repair (Thoracotomy):
Q3: What are the technical considerations in planning this case?
Planning for the management of a traumatic aortic injury, especially with TEVAR, involves several critical technical considerations:
A1:
BTAI with acute type B AD of the DTA zone 3 to 4
A2:
Medical ttt with permissive hypotension syst bl pr not more than 80 HR less than 60 bpm
OSR lat thoracotomy
TEVAR is of choice according to EVES guidelines
A3:
Access site the ptn is young age with small vessels so he may need a conduit to deliver the system as the smallest delivery syst profile is 16 with a minimum fem diameter 6 mm
Prox landing zone from the LSA at least 2 cm
Entry site of the intimal flap
Distal landing zone
Diameter of the aorta in young ptn as long as the smallest device available in the market 21 can be used for aorta 16 mm
A1..
The most likely diagnosis is traumatic aortic dissection acute type B complicated by shock
A2..
For this case
Options of treatment are
At first resuscitation with following the permissive hypotension protocol
Once he is resuscitated optimum blood pressure control is a must so as not to deteriorate dissection from high blood pressure
Repaire of tear by either TEVAR. Or OSR
A3..
For this young man with traumatic dissection of thoracic aorta it is important during planning for repaire to consider
Landing zones cto be in a clear area from dissection with at least 2 cm landing zones
Possibility of aortic branch vessel coverage and if there a need for pre or post operative revascularization
If there is a malperfusion syndrome and a need for branch vessel revascularization
Graft type and size to fit with such a small aortic diameter and the possibility for aortic growth later on