
News & Events
Wave 2: Module 3: Aortic Week 5 – Case 2
73 year old female, presenting with acute chest and interscapular pain that started 2 hours ago. Had one episode of collapse and brought to hospital via ambulance.
Background history of HTN, IHD and is a current smoker
CT Aortogram shows a ruptured descending thoracic aortic aneurysm:
Diameter of thoracic aorta at Zone 3 = 30.6mm, Diameter of thoracic aorta at Zone 5 = 33mm
Q1: What is your initial management plan?
Q2: What are the technical considerations and challenges for an endovascular repair in this case?
Intra-operative findings:

Q3: What would you have done differently?
Q4: How would you rectify this issue?
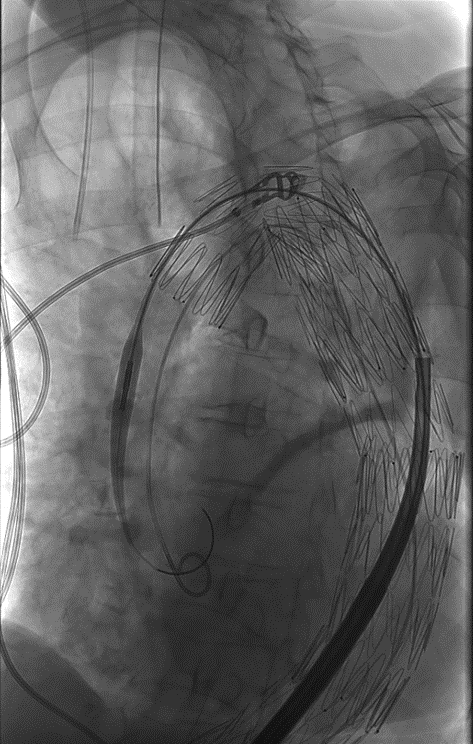
This is the final image after completion of the repair
Q5: What are your post-operative concerns?
Q6: How would you manage this patient in the immediate post-operative period?
7 Comments
Leave a Reply
You must be logged in to post a comment.
A1
Start resuscitation
Keep pt in permissive hypotension
Arrange for urgent tevar
…..
A2
Deploy the stent graft quickly with proximal landing zone at least 20 mm from the lt subclass a
During deployment, need to control bp to avoid migration
Check distal landing zone and make sure the access vessel are suitable
….
A3
stent graft migration especially if the proximal landing zone wasn’t well covered
……
A4
Need to use another stent graft to properly cover the proximal landing zone and seal leak
……
A5
There’s risk of upper limb ischemia
Or even spinal cord ischemia ,depending on collateral
……
A6
We monitor perfusion of lt upper limb and forspinal cord perfusion
We keep MAP >80
Put prison semiseting for 48 hrs
Do csf drainage
Aim to keep sat above 95%
Q1:
Start resuscitation, keep the patient in permissive hypotension, and meanwhile arrange for urgent TEVAR as fast as possible.
⸻
Q2:
Deploy the stent graft quickly with a proximal landing zone at least 20 mm from the left subclavian artery. During deployment, we need to control the blood pressure to avoid migration. Also, check the distal landing zone and make sure the access vessels are suitable in diameter.
⸻
Q3:
One complication is stent graft migration, especially if the proximal landing zone wasn’t well covered. Sometimes ballooning is tried, but it might not solve the issue.
⸻
Q4:
In that case, we may need to use another stent graft to properly cover the proximal landing zone and seal the leak.
⸻
Q5:
If the left subclavian artery is covered, there’s a risk of upper limb ischemia, or even spinal cord ischemia, depending on the collateral supply.
⸻
Q6:
We monitor perfusion of the left upper limb, and for spinal cord protection, we keep MAP > 80, put the patient in a semi-setting position for 48 hours, and if needed, do CSF drainage. Also, we aim to keep oxygen saturation above 95% all the time.
A1: Immediate resuscitation with permissive hypotension
A2: Rapid and accurate device deployment distal to the LSA.
A3: Intraaortic ballon dilatation might cause distal migration of graft
A4: using another stent graft to cover the proximal landing zone and avoid migration
A5: Covering the LSA might cause upper limb ischemia and spinal cord ischemia.
A6: Oxygen SO2 above 95
Close monitoring of the ul perfusion by pulsoximetry
Q1:
resuscitate and permissive hypotension and arrange for emergent TEVAR
Q2:
Rapid deployment of the device with proximal landing zone 20mm from left SCA
control of BPr during deployment to avoid migration
distal landing zone and diameter of the accessed vessel
Q3:
stent graft migration after improper coverage of the proximal landing zone and trial of ballooning
Q4:
using another stent graft to cover the proximal landing zone
Q5:
coverage of the left SCA and possibility of ul ischemia
or Spinal cord ischemia
Q6:
monitoring of the left UL perfusion
spinal cord protection by maintaining of MAP above 80
put the patient in semisetting position for 2 days CSF drainage if needed
O2 saturation above 95
A1: Initial Management Plan
ATLS with patient resuscitation.
A2: Technical Considerations and Challenges for Endovascular Repair
A3: What Would You Have Done Differently?
Avoid intra-aortic balloon inflation against pressure, as it can lead to distal migration of the graft, especially due to a gothic arch with an acute angle.
A4: How Would You Rectify This Issue?
Perform another proximal stent graft extension to address the migration, ensuring a sufficient landing zone.
A5: Post-Operative Concerns
Following the extension stent that covers the LSA, primary concerns are upper limb (UL) ischemia and spinal cord ischemia (SCI).
A6: Immediate Post-Operative Management
A1:
ATLS with ptn resuscitation permissive hypotension cautous fluid replacement
Iv b blockers emergent OR for ttt of r DTA with TEVAR
A2:
Time management to rapid deployment of the device accurately just distal to the LSA
The origin of LSA prox landing zone more than 20 mm
Bl pr control during the deployment not exceed 80 to 90 sbp
Distal landing zone
Access site diameter
A3:
Intra aortic moulding ballon inflation against pressure cause distal migration of the graft because of gothic arch with acute angel
A4:
Another proximal etent graft extension to treat the migration with enough landing zone
A5:
After the extention stent that cover the LSA we are fear of UL ischemia and SCI
A6:
Close monitoring of the ul perfusion by pulse or pulsoximetry
SC protection by MAP above 80 ptn in semi setting for 2 days SCF drainage may be needed CVP less than 15
Oxygen so2 above 95
A1..
Initial management plan is to resuscitate the patient with permissive hypotension protocol
Obtaining blood samples for cross matching and preparing for urgent TEVAR
A2..
For a case of ruptured DTAA the ongoing bleeding and shock state are a challenging technical situations that require high experience
Without pre op aortogram it require proper sizing depending on intra operative aortography
Aortic anatomy and angle of the arch and precise deployment of the stent graft all are technical challenges
The on shelf available devices
A3..
I think I had deployed the stent graft inaccurately before rupture site
A4..
Extension of the stent graft in a more proximal zone
A5..
I will concern about spinal cord ischemia, since I had covered the SCA to get her with thorathic aortic stent graft
A6..
In the immediate post operative period I will keep the systolic blood pressure high with mean arterial pressure above 90 mmHg
I will keep the patient lying flat on bed for 72 hours
I will keep spinal fluid pressure below 10 mmHg by spinal fluid drainage