
News & Events
Wave 2: Module 2: Lower Limb – Week 8 – Case 2
1- IVDU, PSA, ligated femoral artery, dead leg
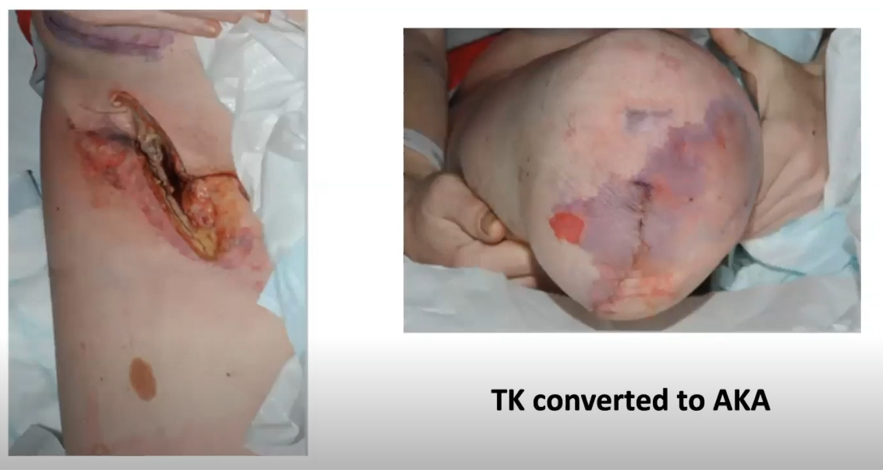
What happened to this stump and why?
Would you have done the same to begin with and why?
2- DM, PAOD, the patient declined BKA

What do you learn from this story depicted in pictures?
How do you implement shared decision making?
7 Comments
Leave a Reply
You must be logged in to post a comment.
Case 1
Ischemic stump due to vascularity defect
Starting 1 st with trial of revasculrizaion and in case of emergent amputation high above knee proceeded
————
Case 2
Distal amputation is prefered
Long lever better than short one
###Case one .
A..>>
Ischemic infected stump
Due to ligation if CFA and PFA in the setting of infection
B ..>>
I will not start with TN amputation as the stump will be ischemic I will do amputation as high as possible and I will not close the stump at first till I am sure that it is clean with dressing
###Case two ..
A..>>
I learned not to jump to amputation untill every effort had been done specially when vascularity is good
B..>>
A1 ischemic infected stump due to ligation of CFA and profunda
A2i will try to spare profunda or do extra anatomical bypass to ensure good blood supply
I will do aka as high as possible
case 2
A1 respect patient decision
give patient try when he has good vascularity
and willing to stick to his meds and dressing
2 it is a group decision between patient and physician
we should give patient his trail if good vascularity and willing to save his limb
Case(1):
1- Ischemic infected stump….due to ligation of the comon femorala and profunda femoris arteries.
2- I will try to spare the profunda femoris artery to preserve the blood supply of the thigh.
Case(2):
1- To be patient not to begin with major amputation and perform extensive debridment, watch and see results of debridment as the wound may heel.
2-Team consultation is important and to respect the patient’s desire.
Case(1):
1- Ischemic infected stump….due to ligation of the comon femorala and profunda femoris arteries.
2- I will try to spare the profunda femoris artery to preserve the blood supply of the thigh.
Case(2):
1- To be patient not to begin with major amputation and perform extensive debridment, watch and see results of debridment as the wound may heel.
2-Team consultation is important and to respect the patient’s desire.
Case one .
A..
Ischemic infected stump
Due to ligation if CFA and PFA in the setting of infection
B ..
I will not start with TN amputation as the stump will be ischemic I will do amputation as high as possible and I will not close the stump at first till I am sure that it is clean with dressing
Case two ..
A..
I learned not to jump to amputation untill every effort had been done .
B..
The patient decision should be respected . And decision should be for the team not only one person
Ischemic stump beaause of common femoral artery ligation
Try to preserve profunda when ever possible
Second case
Respect patient demands And good counseling of the patient And staged decisions may do benifts