
News & Events
Wave 2: Module 2: Lower Limb – Week 8 – Case 1
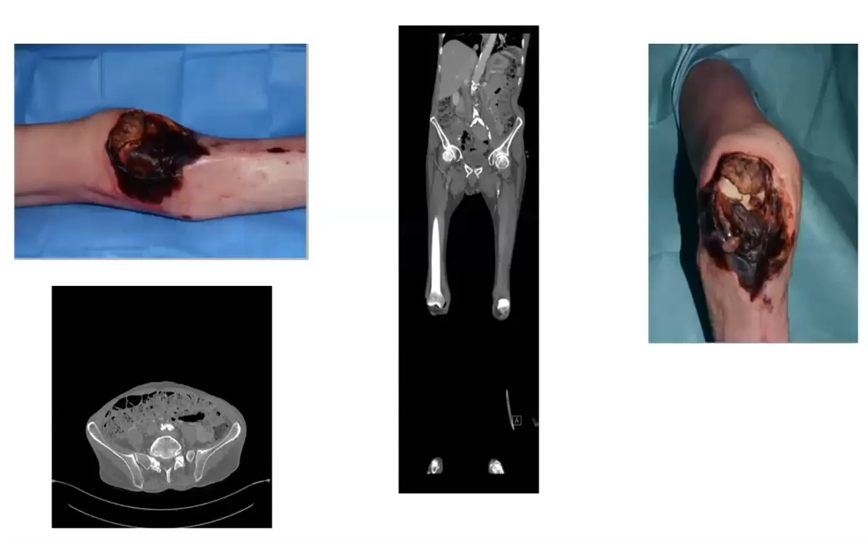
1- DM, neuropathy, IHD, war veteran and contralateral below knee amputation

What investigations?
How do you manage this ulcer?
Any room for preserving the limb?
How do you council the patient?
2- Cachectic, self-neglect
What do you want to do to this patient?
Can you salvage the limb and why?
What do you think the patient’s best interests are?
10 Comments
Leave a Reply
You must be logged in to post a comment.
Case 1
1
CBC,HBA1C ,LFT,RFT
DUPLEX AND CTA
XRAY ON THE BONE
2. If there is No OM ,only infection..partial calcenectomy and offloadinfg will be beneficial
3.
_____
Case 2
1. Let femoral angiolplasty then AKA
2. No..lost knee (Dead limb)
3. Temination of pain , getting rid of sepsis
Case 1
Q1 Investigation::
Lap : cbc-pt-ureacreat-k-hba1c- lipid profile
Rad : duplex arterial- cTA
Q2
Revascularization
Anti plt
Anti coagulant
Q3
Trial of revascularization then debridement
Q4
Informing pt with risk
Ttt option
Out come of operation
Timing and duration of operation
——————
Case 2
Q1 resusitation
Stabilization of general condition
Prepare for AKA
Q2
Difficult for salvaging as necrosis extending into deep tissue of knee joint
Q3
Relief of pain
Improve of general condition
###Case (1):
Q1
Q2
In case of intact distal pulses: Extensive debridment up to partial calcenectomy.
In case of peripheral arterial disease and osteomyelitis: major amputation.
Q3
partial calcenectomy and offloading, but it may end with major amputation.
Q4
###Case(2):
Q1
Trial of angioplasty to restore the left common femoral artery then LT AKA to save the stump.
Q2
No, it is non-salvagable due to exposure of the bone with severe foot infection in addition to Aortoiliac occlusive disease.
Q3
Termination of pain and getting rid of the cause of sepsis.
A1 investigation
cbc -kidney function test -coagulation profile -crp
imaging x-ray foot to show osteomyelitis
duplex and CTA to show vascularity if no pulse felt
A2 if good vascularity extensive debridement of heel with off loading
if no peripheral vascularity offer patient major amputation
A3 if good vascularity we will give a try to preserve the limb
A4 I will tell the patient it is a trail to reserve the limb which may take a long time of dressing to got healed
and it may end up with major amp
case 2
A1 first we need to revscularise profunda artery to ensure good supply for aka stump
A2 no this patient needs a major amp according to his ulcer site and fixed knee joint
A3 his best interest is pain relief and ensure there is no sepsis risk
Case 1:
Q1 foot xray, and arterial duplex
Q2 and Q3 if there’s no osteomyelitis and intact distal pulse, extensive soft tissue debridement, if there’s osteomyelitis and intact distal pulse extensive debridement plus partial calcenectomy, if there’s major osteomyelitis and impaired vasculature then bka
Q4 my main councilling will be about it’s all a trial to save the limb with no great expectations.
________________________
Case2:
Q1 angioplasty to restore femoral pulse then aka
Q2 i don’t think it is salvageable as the knee joint is non functional
Q3 pain relief
Case (1):
1-CBC, coagulation profile, renal function tets,arterial duplex U/S if distal pulses not felt and maybe CT angiography.
Plain X-ray foot to detect osteomyelitis and tissue infection.
2- In case of intact distal pulses: Extensive debridment up to partial calcenectomy.
In case of peripheral arterial disease and osteomyelitis: major amputation.
3- partial calcenectomy and offloading, but it may end with major amputation.
4- It is a trial to save the limb as it is a precious one =, so aggressive debridment must be done …It may end up with major ampuation.
In that case physiotherapy and wearing prothesis should be arranged for proper rehabilitation.
Case(2):
1-Trial of angioplasty to restore the left common femoral artery then LT AKA to save the stump.
2- No, it is non-salvagable due to exposure of the bone with severe foot infection in addition to Aortoiliac occlusive disease.
4- Termination of pain and getting rid of the cause of sepsis.
Case (1):
1-CBC, coagulation profile, renal function tets, ABPI, arterial duplex U/S if distal pulses not felt and maybe CT angiography.
Plain X-ray foot to detect osteomyelitis and tissue infection.
2- In case of intact distal pulses: Extensive debridment up to partial calcenectomy.
In case of peripheral arterial disease and osteomyelitis: major amputation.
3- partial calcenectomy and offloading, but it may end with major amputation.
4- It is a trial to save the limb as it is a precious one =, so aggressive debridment must be done …It may end up with major ampuation.
In that case physiotherapy and wearing prothesis should be arranged for proper rehabilitation.
Case(2):
1-Trial of angioplasty to restore the left common femoral artery then LT AKA to save the stump.
2- No, it is non-salvagable due to exposure of the bone with severe foot infection in addition to Aortoiliac occlusive disease.
4- Termination of pain and getting rid of the cause of sepsis.
Case 1:
A1: labs including cbc hba1c crp esr prep for op fitness
Imaging in the form of xray for the bone condition OM air FB together with arterial duplex or CTA for blood supply evaluation if he has no pulses
A2: preserving surgery in the form of debridement and partial calcenectomy to be cosidered regarding the contralat BKA
A3: foot preserving option although it will take time and at the end it may end with higher level of amputation
Case 2:
A1: as long as he has ishemic limb with iliac lesion it is better to be revascularized by angioplasty to secure femoral pulse for the AKA stump survival
A2:
This limb is non salvageable because of opened joint capsule with exposed fem condyles
A3:
The ptn best interest is to be pain free as he is cachectic so function wouldnt be acheivable
Case one
A ..
Lab …CBC, CRP, and ESR
radiology .. x-ray and Arterial duplex
B..
It is a precious limb so efforts should be done to save the limb
If it is only infection debridment of bone and soft tissue should bt tried firstly
C..
Yes, partial calcenectomy and offloading
D.. it is just a trial to save the limb with depridement but it may fial and end with limb amputation
Amputation is not the end of the story but it could be the beginning by proper rehabilitation
Case two
A …
For this patient .. AKA
B..
It is an AIOD and limb salvage needs a revascularization procedure and in a cachictic and a self neglected patient it is a risky operation and amputation is better for him
C..
This patient bast interest is to get rid off the necrotic tissues and pain relief
First case
ABI assessment+lab+CRP+x-ray calcenous
If only Df infection with good vascularity no osteomyelitis
For surgical debridement
If pad+osteomyelitis for amputation
Beter function Equal better Life
Second case
For aka
No because of function less knee
Pain relief